Comparison of LINAC equipped with either OBI/CBCT or
Almon Shiu, Ph.D.
The
Introduction: Clinical outcome of radiotherapy can potentially be improved by increasing the precision of tumor localization and dose delivery during the treatment. Various image-guided radiotherapy delivery systems are now available to achieving the goal. The purpose of this study is to investigate the relative advantages and limitations of the OBI/CBCT (Trilogy) vs. Varian LINAC/CT-on-rails unit with a 6D robotic couch top for image-guided radiotherapy (IGRT).
Method and Materials: Optimal
image-guide radiotherapy (IGRT) delivery system should be capable of handling
the auto setup of the updated isocenter with 6D corrections, the adaptive
radiotherapy, and treating multiple lesions simultaneously. The CT image
quality should be suitable for designing a treatment plan. The planning CT and
the daily CT are acquired in the treatment setup condition, minimizing any
systematic errors coiled into the image-data. A 60-cm diameter of maximum
field-of-view (FOV) is crucial to scan almost all the patient population in US.
The scanning-range in superior-inferior direction should cover the maximum treatment-field
length available on the radiotherapy delivery system. It should have KVp and MV portal-imaging capabilities for setup 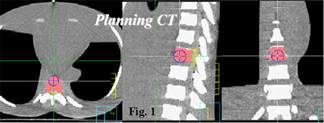 verification.
Monitor the target-isocenter shift due to couch rotation. A thoracic phantom
was used to evaluate the IGRT setup accuracy using either the OBI/CBCT or the
CT from LINAC/CT-on-rails unit. The planning CT images were acquired from the
LINAC/CT-on-rails unit. A treatment plan was generated from a clinical
treatment planning system and is shown in Figure 1. Then, the thoracic phantom was setup at
Trilogy and LINAC/CT-on-rails with similar conditions; the shifts and rotations
were applied to the phantom to test the accuracy of aiming the target
accurately on Trilogy and on LINAC/CT-on-rails unit. The in-house
image-registration software was used for both tests to ensure a fair comparison
in our study.
verification.
Monitor the target-isocenter shift due to couch rotation. A thoracic phantom
was used to evaluate the IGRT setup accuracy using either the OBI/CBCT or the
CT from LINAC/CT-on-rails unit. The planning CT images were acquired from the
LINAC/CT-on-rails unit. A treatment plan was generated from a clinical
treatment planning system and is shown in Figure 1. Then, the thoracic phantom was setup at
Trilogy and LINAC/CT-on-rails with similar conditions; the shifts and rotations
were applied to the phantom to test the accuracy of aiming the target
accurately on Trilogy and on LINAC/CT-on-rails unit. The in-house
image-registration software was used for both tests to ensure a fair comparison
in our study.
 Results: the current CT image quality
of CBCT is suitable only for image registration. However, the relative large
intra- and inter-variation of CT numbers for the same tissue inhibits the use
of CBCT for treatment planning and the adaptive radiotherapy. The single
scanning-range of CBCT is limited to 14 cm. Both scanners need to increase the
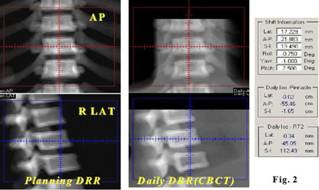
FOV to 60-cm diameter. The results of image registration between the planning
DRRs and the CBCT DRRs are shown in Figure 2. It shows the phantom had 0.75° CW
roll (viewing from the foot), the 1° CW yaw (viewing from the beam direction)
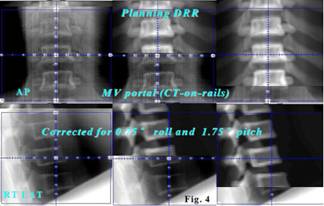
and 2.5° tilt down towards the gantry side. Figure 3 shows the verification of
the AP and RT LAT planned DRRs and the KVp AP and RT LAT portal images in
horizontal and vertical split screens. It aimed isocenter correctly but could
not handle the rotations in the setup (No mechanism is available now to correct
the rotations except the roll). However, the similar study on the
Results: the current CT image quality
of CBCT is suitable only for image registration. However, the relative large
intra- and inter-variation of CT numbers for the same tissue inhibits the use
of CBCT for treatment planning and the adaptive radiotherapy. The single
scanning-range of CBCT is limited to 14 cm. Both scanners need to increase the
FOV to 60-cm diameter. The results of image registration between the planning
DRRs and the CBCT DRRs are shown in Figure 2. It shows the phantom had 0.75° CW
roll (viewing from the foot), the 1° CW yaw (viewing from the beam direction)
and 2.5° tilt down towards the gantry side. Figure 3 shows the verification of
the AP and RT LAT planned DRRs and the KVp AP and RT LAT portal images in
horizontal and vertical split screens. It aimed isocenter correctly but could
not handle the rotations in the setup (No mechanism is available now to correct
the rotations except the roll). However, the similar study on the
Conclusions: Based on the image
registration, LINACs equipped with either OBI/CBCT or